What Shingles and Covid Have in Common
And Why Yale Epidemiologist Dr. Harvey Risch says Alex Berenson is Wrong
My friend Beth had Shingles several years ago. She woke up one day to discover a mysterious rash wrapped around her torso and immediately saw a doctor, who quickly diagnosed the condition and prescribed an antiviral. We were both surprised to learn that an effective antiviral existed for Shingles. Neither of us could recall ever having seen any ads for such a drug.
By contrast, we’ve seen public health campaigns promoting the Shingles vaccine for many years. We also regularly come across advertisements for that vaccine at our local pharmacies and supermarkets.
Because of the risk of autoimmune disease inherent with all vaccines, I take none of them. Therefore, these ads don’t benefit me.
After confirming a Shingles diagnosis, the doctor instructed Beth to go directly to the pharmacy and pick up an antiviral prescription. The medicine, he warned, must be started in the first few days of illness to be effective. He was right.
From WebMD:
Beth followed the doctor’s advice. Her Shingles was painful but resolved quickly without incident.
A couple years later I noticed what felt like a small insect bite behind my left ear. Assuming Shingles appeared only on the torso, I did not suspect it. Two days later I noticed a rash developing on the same side of my head, along my jaw line. Simultaneously my head began to throb. A relative saw the rash and immediately suspected Shingles. I looked it up and learned that, in fact, while the Shingles rash commonly appears on the torso, it can also form on other parts of the body, including the arms, face, and scalp. I learned that if Shingles infects the face or scalp, it can reach the eye. One possible complication is loss of vision!
Knowing I had not a moment to waste, I picked up the phone and called my doctor. Within hours he was examining my rash, confirming the diagnosis, and calling in an antiviral prescription for me. He advised me to go straight to the pharmacy to pick it up. He also instructed me to be sure to take all three doses that first day (the daily regimen was three doses), even though by then it was already mid-afternoon.
I did as my doctor instructed. My condition steadily improved over the next week and resolved without incident.
Shingles thus served as my personal tutorial on the importance of early intervention when treating a virus with antivirals. The point is to prevent the virus from replicating. Once it has replicated and spread within the body, an antiviral serves little purpose. This concept seems rather elementary. It is something that virtually anyone with even limited education should be able to understand.
That’s why, when the FDA announced in the spring of 2020 that Covid patients would only have access to the stockpile of hydroxychloroquine (HCQ) when hospitalized, I began to suspect that something was terribly wrong. In February of that year, I had read the first reports that South Korean doctors were using HCQ to treat Covid-19, with good results. HCQ in combination with Zinc was acting as an antiviral.
Why were Americans being denied outpatient antiviral treatment for Covid-19? Who would benefit by waiting until patients were already so sick that they required hospitalization? Wouldn’t it already be too late for many patients by then?
While the first two questions have yet to be adequately addressed by anyone, of course the answer to third question is yes.
Fast forward two years and, despite many studies now showing that both HCQ and Ivermectin are effective antivirals for Covid, we are still being treated to a parade of horribles in the form of media reports and published studies claiming these medications don’t work.
The Definition of “Early”
The latest comes from Malaysia. It is a randomized, controlled study published in the prestigious Journal of the American Medical Association (JAMA) comparing outcomes in 490 Covid patients, approximately half of whom received “treatment during early illness” with Ivermectin while the other half received “standard care” (i.e., no antiviral). The authors concluded that Ivermectin offered no benefit to Covid patients. [1]
Subsequent to its publication, numerous doctors and Substack writers pointed out that only three people died in the Ivermectin group versus ten in the control group, but the difference was too small to reach statistical significance because the study itself was too small, with too few patients in either group who succumbed to death.
Other critics of the study noted that patients in the treatment arm were not given Zinc.
Still others, including Dr. Pierre Kory, emphasized that most patients in the study did not receive their first dose of Ivermectin until at least the fifth day of symptoms.

While the study accepted patients with both mild and moderate disease severity, 323 patients (two-thirds) were in the latter category. Substack writer Igor Chudov noted that nearly all 323 of these patients had presence of Covid-19 lung changes upon enrollment. He wrote:
“… is it surprising that 52 out of 158 patients in the ivermectin group, and 43 out of 165 control group members, who had bad lung radiography, proceeded to the “severe stage” shortly after admission?” [2]
Furthermore, 19 patients in the subgroup analysis of patients with severe disease were enrolled in the trial and started on Ivermectin more than five days after illness onset.
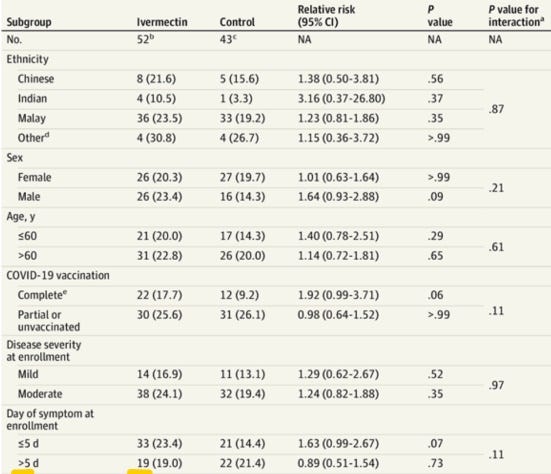
The study doesn’t tell us whether the four patients in the Ivermectin group who eventually required a ventilator, and the three who died, were among those 19 patients.
What the study does reveal, but then ignores, is that among the patients in both groups who progressed to severe disease, those who received Ivermectin did better, even though they did not receive the drug “early” in their illness as the authors claimed and were not given Zinc.

I spent a chilly Presidents Day with family watching Monk reruns. If patients in the Malaysian study had decided to watch a Monk marathon while waiting for Covid treatment, the average febrile, coughing, shivering, aching patient in the treatment arm of the study would have watched the “defective detective” solve 144 crimes (including 19 of them twice) before swallowing his/her first dose of Ivermectin. This study that claimed to be testing Ivermectin as an early treatment for Covid clearly was not.
Regardless, CNN pounced on the study as definitive proof that Ivermectin offers no benefit to Covid patients.
So did Alex Berenson. He wrote, “To the Ivermectin Fanatics… Just stop, okay? One good randomized trial is worth 100 observational studies, and this was a good randomized trial. It set a reasonable endpoint and it missed. It didn’t just miss, it trended negative. So the secondary endpoints don’t mean squat.” [3]
Among the “secondary endpoints” that Berenson claimed didn’t mean squat was the 70 percent lower death rate in the Ivermectin group.
Here’s What Happened
From the outset, Berenson has taken a hard line on studies of early treatment, asserting that only randomized, controlled trials (RCTs) can prove the efficacy of these drugs. Literally hundreds of studies have now been published showing efficacy for both HCQ and Ivermectin in Covid-19, but none of the trials or studies with the strongest evidence in favor of these treatments are RCTs.
Berenson’s excellent work exposing serious problems with the government’s pandemic response has earned him a large following, deservedly so. Yet, he has dismissed – at times rather rudely – doctors and patients (including his own readers) who say these drugs are saving lives and should be made available to everyone on an outpatient basis.
On Jan. 14, 2022, Berenson was paired with Dr. Robert Malone on Fox News to discuss censorship. He instead used the segment to trash not just Ivermectin but Malone for promoting it. Berenson subsequently hopped on Substack to defend his attack on Malone. He promised to have more to say on Ivermectin soon:

That was more than one month ago. Berenson published many articles in the interim but not a single word about Ivermectin.
Then last week the Malaysia study came out, and Berenson quickly seized upon it to settle the score.
Berenson is a Yale graduate. He holds degrees in history and economics. Impressive.
Dr. Harvey Risch, MD, PhD, is Professor of Epidemiology in the Department of Epidemiology and Public Health at the Yale School of Public Health and Yale School of Medicine. He holds a medical degree and a PhD in mathematical modeling of infectious epidemics.
When asked for a list of the most compelling studies of HCQ and Ivermectin as early treatments for Covid, Dr. Risch told me via email:
“Citing select "compelling" studies is not science, it is cherry-picking… HCQ is virtually proven to reduce risk of mortality when started during the first few days of Covid illness…The evidence for IVM [Ivermectin] is also good, though not as extensive as for HCQ. Berenson assumes that RCTs must mean something. He doesn't understand how easy it is to subvert RCTs and is wrong.”
Risch’s extensive summary of the evidence in support of Covid early treatment with HCQ is here:
https://earlycovidcare.org/wp-content/uploads/2021/09/Evidence-Brief-Risch-v6.pdf .
An up-to-date list of HCQ studies is here:
COVID-19 early treatment: real-time analysis of 1,482 studies (c19early.com)
An up-to-date list of Ivermectin studies is here:
Ivermectin for COVID-19: real-time analysis of all 148 studies (c19ivermectin.com)
Risch also pointed me to an excellent presentation he gave last summer on HCQ and the drug industry-driven effort to discredit non-randomized trials. [4] In it, he explained that “small, randomized trials that you see of 100 or 200 or 500 people are useless. They’re no better than non-randomized trials on the basis of randomization.” He said researchers should use whole bodies of scientific knowledge in evaluating treatments. “This is how science is done, not by randomized trial fetishism.”
The entire presentation is worth listening to. Below are four screenshots that capture some of the highlights:




Risch said the FDA is flagrantly ignoring the 2016 law that requires federal agencies to use other forms of evidence in addition to or in place of randomized trials.
Serving Big Pharma, Not Patients
With its telltale rash, a virus like Shingles is much easier to spot quickly, provided people know what to look for. By contrast, the symptoms of Covid can mirror those of other viruses. The countries that have successfully tamed Covid with HCQ or Ivermectin have done so by distributing packets containing one of the two drugs to their populations wherever the virus is raging, and instructing people to begin taking the medicine, along with Zinc, at the first sign of illness. [5] Since these drugs are very safe, officials in those countries reason, there is no harm in taking them even if the illness turns out to be something other than Covid.
To date, doctors in the U.S. have been unable to convince our government to do the same, for the obvious reason that doing so would drastically reduce demand for the vaccines. The pharmaceutical industry pushes profitable vaccines that can be given to everyone over cheap generic drugs that will be needed only by sick people. The FDA and CDC, which are captured by the industry, assist in this effort.
Patients obviously are ill-served by a strategy that markets vaccines to the exclusion of all other medical interventions. The U.S. no doubt would experience far superior health outcomes if some of the millions of dollars spent pushing vaccines were instead allocated to public service announcements designed to teach the public how to recognize the early signs of Shingles, Covid and other common viruses for which effective early treatments are available. Public health authorities who profess to actually care about health should make these treatments easily accessible to the entire population rather than aiding and abetting the drug industry’s efforts to trash them.
Thank you for reading. If you like this article, please share it with your friends, family and colleagues.
I would also like to hear your thoughts.
[1] Efficacy of Ivermectin Treatment on Disease Progression Among Adults With Mild to Moderate COVID-19 and Comorbidities: The I-TECH Randomized Clinical Trial | Complementary and Alternative Medicine | JAMA Internal Medicine | JAMA Network
[2] Malaysia Study: Ivermectin helps with "Covid Lungs" (substack.com)
[3] To the ivermectin fanatics - by Alex Berenson (substack.com)
[5] COVID cases in Indian Uttar Pradesh drops by 97.1 percent because of Ivermectin use - Weekly Blitz
Thank you for this. I stopped following Berenson after his destructive, unwarranted, ill-conceived, malicious & just plain stupid character assault on Dr. Malone.
A word on shingles. 2 decades ago broke out in the torso rash. I guessed what it was, but had jury duty so grabbed my herbal books to read during wait times. Was thrilled to discover that I had growing in my garden all I needed...When I got home I made a very strong infusion of every mint family plant I had, from oregano to catmint. I strained out the leaves & drank the "tea" throughout the day. I bandaged my torso with the strained leaves, wrapped in cotton batting sprinkled with cayenne pepper. I covered the cotton with a piece of plastic wrap, then a horse bandage around the outside to hold it all in place.
I was able to work both office & minifarm. Iirc it resolved within a week. I had the distinct sense that had I been able to treat from onset, it would have been resolved in half that time.
Less convenient than pills, but free, educational & self-empowering!
Excellent. Very informative!